Concha Bullosa symptoms and treatment: How I explain it to my patients
Last Tuesday, a patient sat across from me with tears in her eyes. “Doctor, I’ve seen three specialists and no one can tell me why I can’t breathe through my nose.” She had tried different medications for years, yet the blockage kept coming back.
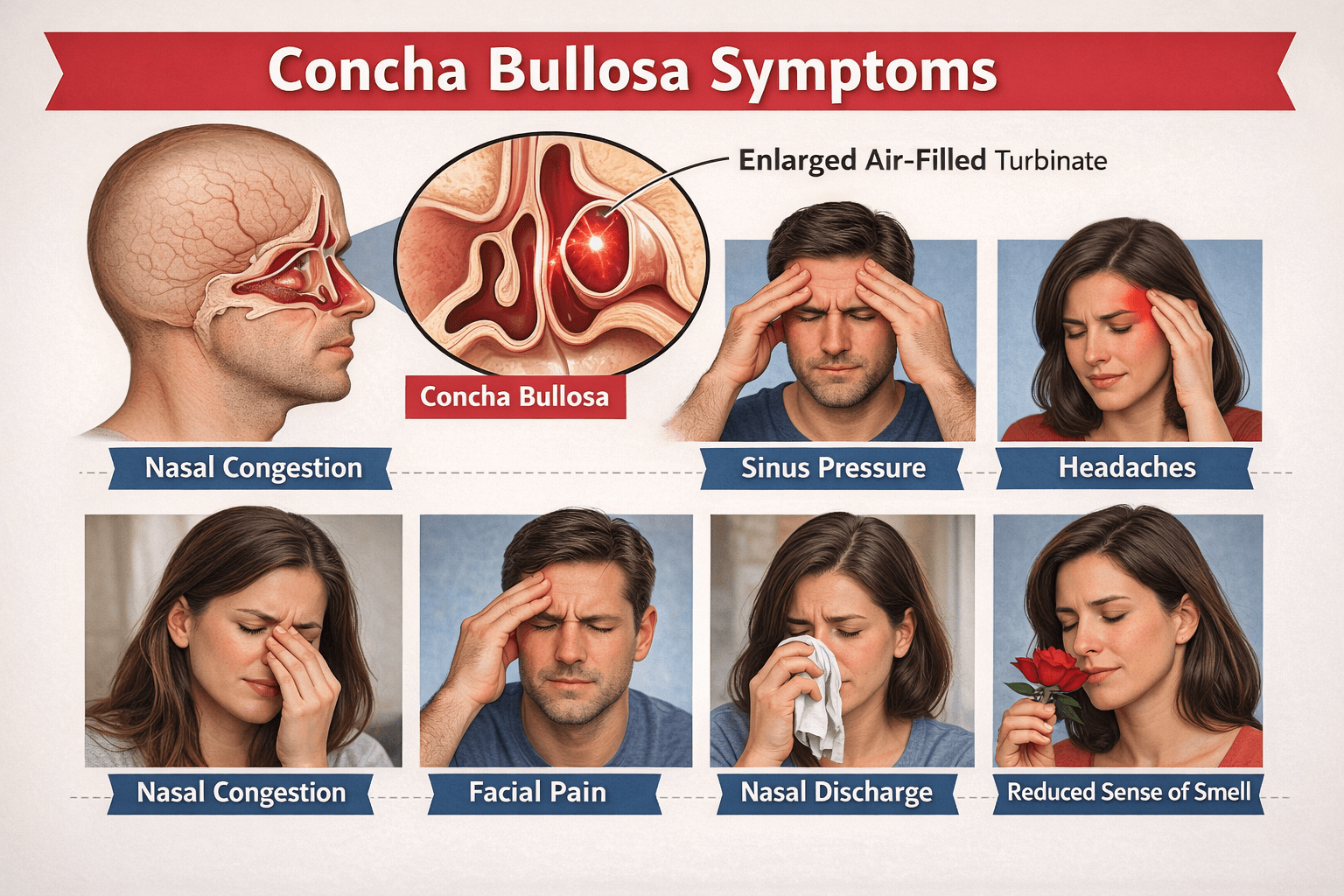
I pulled up her CT scan. After about thirty seconds, I pointed to a small air pocket inside one of the turbinates in her nasal cavity. “This,” I said, “is called concha bullosa, and it’s been hiding in plain sight.”
Concha bullosa symptoms can look like other causes of nasal obstruction, including allergies, chronic congestion, and even “just sinus problems.” When you feel pressure, headaches, post-nasal drip, and poor sleep from mouth breathing, it is easy to blame the usual suspects.
But sometimes the root cause is a pocket of air inside a turbinate that changes airflow and drainage.
What I tell patients about Concha Bullosa
When I say “turbinate,” many patients picture something scary. It is not. Turbinates are curved structures inside your nose. In medical literature, turbinates help with:
- hydration
- lubrication
- arranging airflow
- filtration
- smell
- thermoregulation
Turbinates help condition the air you breathe, and they guide airflow so your nose works like it should.
Now let’s talk about concha bullosa.
A concha bullosa is pneumatization of a turbinate. That means there is an air cell inside the turbinate. Many people hear “air pocket” and assume it must be an infection. It may not be. Sometimes it is just a normal variation that sits quietly for years.
The “balloon effect” I describe in the exam room
This is the picture I use: imagine a turbinate that has a small hollow space inside it. If that space gets larger, the turbinate can become bulky, almost like a ballooned area within the nasal passage. When that happens, it can narrow the airflow channel and can also get close to nearby structures.
Patients often ask, “Was I born with this?”
The exact cause is not fully known, and some literature describes several hypotheses.
- One is that sinus pneumatization expands into the turbinate during the intrauterine period.
- Another is a fusion abnormality during fetal development.
- A third idea involves microfractures in the turbinate during late puberty, which may allow mucosa to invaginate and form the bullosa cavity.
So yes, it can start early, and symptoms may show up later. That timing is one reason patients feel confused. They may have breathed “fine enough” for years, then slowly notice worsening blockage and pressure.
The analogy I use when patients feel stuck
When someone feels like air will not pass through one side of the nose, I often use my “garden hose with a kink” example.
Water still moves, but it struggles. In the nose, airflow still moves, but it becomes turbulent, weaker, and sometimes frustrating. People compensate by mouth breathing, especially at night. Then sleep quality drops, and fatigue rises.
And here is another reason it gets missed. Concha bullosa is often found incidentally on imaging. It can look like “just anatomy” until it is large enough, inflamed, or positioned in a way that blocks key pathways.
The Concha Bullosa symptoms I see most often in my practice
Symptoms can vary because concha bullosa can affect different turbinates. It is most common in the middle turbinate, and it is rare in the inferior turbinate. Still, any turbinate can be involved, and sometimes more than one is pneumatized.
One big pattern I listen for is whether symptoms are unilateral or bilateral. Some patients can point to one side and say, “This side never opens.” Others feel blocked on both sides.
In a case report, a 33-year-old woman had progressive nasal obstruction on both sides and recurrent headaches for 20 years, with a large middle turbinate concha bullosa extending forward and filling much of the nasal cavity. That kind of history tells me to look beyond routine congestion.
Symptoms that show up again and again
The most common symptom is nasal obstruction.
In a systematic review of inferior concha bullosa cases:
- Nasal obstruction was present in all patients (100%)
- Followed by headache (77%)
- Post-nasal drip (53%)
- Purulent nasal discharge (23%)
In another case report, a 37-year-old woman had nasal obstruction, persistent headache, postnasal discharge, and occasional epistaxis, and she had experienced symptoms for 20 years with poor response to repeated medication attempts.
Patients also describe facial pressure and sinus-type discomfort. Sometimes it feels like chronic sinus symptoms that never fully resolve. People may say the pressure sits between the eyes, in the cheeks, or in the forehead. Others focus on headaches that cycle and return.
Why symptoms get blamed on the “usual” causes
Many people get told they have allergies, “just sinusitis,” or a deviated septum and nothing else.
But concha bullosa can sit beside those issues. There is also discussion in the same literature about a relationship between concha bullosa and septal deviation.
So if a patient has both, it can be hard to tell which one drives the symptoms without good imaging and a careful exam.
Headache is another misdirection. Some experts describe headache related to mucosal contact points. The contact between concha bullosa and adjacent structures may trigger headache through substance P and trigeminal nerve branches. Patients often think this means “migraine” or “stress.” Sometimes that label delays the real concha bullosa diagnosis.
How do you know if your symptoms are from concha bullosa?
I start with pattern and persistence.
If nasal obstruction does not improve enough after a vasoconstrictor spray, and I see turbinate hypertrophy, concha bullosa becomes more likely.
I also look at the whole symptom picture:
- obstruction plus headache
- postnasal drip
- recurring infections
- pressure
- long history despite multiple treatments
Then I confirm it with the right tools. Imaging and endoscopy confirm the diagnosis.
How we confirm Concha Bullosa
I like patients to understand the steps, because a clear plan reduces anxiety. An ENT specialist consultation usually starts with history, then a targeted exam. I ask:
- how long symptoms have lasted
- whether one side is worse
- what treatments have been tried
- what changes with seasons or congestion
Even when symptoms sound “standard,” the timeline often gives clues.
What I look for on physical exam
On nasal exam, I look for turbinate hypertrophy, septal deviation, and mucosal health.
In the case mentioned above, endoscopic exam showed hypertrophy of the inferior turbinates and the right middle turbinate, septal deviation, and unhealthy nasal mucosa.
That combination is common in symptomatic patients, and it is a clue that anatomy and inflammation may be working together.
In the systematic review, inferior turbinate hypertrophy was seen in 92%, middle turbinate hypertrophy in 30%, and septal deviation in 61%. Those are exam findings I keep in mind when I decide what testing is needed.
CT scan
A CT scan is often the clearest way to see concha bullosa. It shows the air pocket and how much space it takes up. In the same case above, CT showed multiple findings, including:
- inferior concha bullosa
- a septated right middle concha bullosa
- bilateral superior concha bullosa
- uncinate pneumatization
- septal deviation
- sinusitis
Treatment choices change when structures communicate with sinuses or when multiple variations appear together.
I also use CT when an area is hard to see on routine exam.
For example, superior concha bullosa can be difficult to reach during endoscopic examination, so CT becomes especially helpful. If a patient’s symptoms suggest deeper contact points or hidden obstruction, imaging gives answers.
Nasal endoscopy
Nasal endoscopy lets me see inside the nasal cavity more directly.
In the same case above, endoscopy showed a large mass with normal mucosa filling the nasal cavity, and CT confirmed it was an extensively pneumatized middle turbinate extending toward the nasal vestibule. That is a perfect example of why endoscopy and CT work well together.
Endoscopy shows what is physically blocking space. CT explains what it is.
When a mass causes unilateral obstruction, it must be distinguished from benign lesions like polyps and from tumorous conditions.
Concha Bullosa treatment options
Not every concha bullosa needs treatment.
Even large ones can be asymptomatic. The key question I ask is simple: are you bothered enough that treatment is worth it?
When symptoms are present, we choose a plan based on severity, anatomy, and response to prior care. Treatment is not needed unless symptoms occur, and medicines like nasal decongestants and corticosteroids can provide relief. That matches what patients often want to try first.
When I recommend conservative steps first
If symptoms are mild, or if the obstruction seems to fluctuate, I may start with medical management.
In the inferior concha bullosa review, some patients were treated medically, some surgically, and some with both. Outcomes were good, and no surgical complications were noted in that review. That tells me there is room to individualize care instead of pushing everyone toward the same path.
At the same time, I set expectations clearly. Medication can reduce swelling and inflammation around the anatomy, but it does not remove the air cell inside the turbinate.
So if the concha bullosa itself is the major blockage, medical care may not be enough long term.
Is surgery always necessary for concha bullosa?
No. Surgery is not automatic.
If a concha bullosa does not cause symptoms, I leave it alone. If symptoms improve with medical care, surgery may not be needed. But when symptoms persist, the literature supports surgery as an effective method for symptomatic cases.
Here is how I explain the decision. If airflow blockage is strong, if drainage pathways are obstructed, or if headaches appear linked to contact points, surgery can give more reliable relief. In the case above, medical treatment did not solve the problem, so endoscopic sinus surgery and septoplasty were done, with additional turbinate procedures. The patient’s complaints healed immediately after surgery.
The surgical techniques I discuss with patients
There are several surgical approaches:
- Crushing and outfracture, often enough for small concha bullosa cases
- Endoscopic resection of the lateral portion of the concha bullosa, which may significantly heal symptoms
- Techniques listed as common conchal surgeries include conchal outfracture, crushing, excision of the free edge of concha bullosa, microdebrider turbinoplasty, and diathermy
- Functional endoscopic sinus surgery and turbinate reduction are also described options
I also explain what not to do.
- Total turbinectomy should not be performed because of risk of atrophic rhinitis.
- And turbinoplasty is contraindicated when an inferior concha bullosa communicates with the maxillary sinus because it may lead to inferior meatal antrostomy and clearance problems.
The safest plan depends on the exact anatomy.
Recovery timeline
Recovery depends on the procedure.
Some approaches are quick and minimally invasive. Surgery is often described as quick and minimally invasive, and follow-ups are guided by your provider. In the same case mentioned above, the postoperative course was uneventful, and at one month the nasal airway looked adequate on endoscopy, with symptoms resolved.
Longer-term outcomes are also described. One study followed patients after endoscopic turbinoplasty for years, reporting low rates of adhesions and no major immediate or long-term complications in their series.
I use information like this to reassure patients who fear that nasal surgery always creates long-term problems. With careful technique and follow-up, outcomes can be very good.
Will insurance cover concha bullosa treatment?
This is a common question in my office.
Coverage depends on your plan and what care is being done, such as:
- imaging
- endoscopy
- medication
- surgery
When a patient needs treatment, my team helps gather documentation from the exam and imaging so the medical need is clearly shown.
During your ENT specialist consultation, I encourage you to ask about costs early so there are no surprises later.
Final words
Concha bullosa symptoms can feel mysterious. You may have nasal obstruction that never fully clears, headaches that keep returning, postnasal drip, chronic pressure, and recurring infections that do not respond to the usual steps. Because these symptoms overlap with many nasal obstruction causes, concha bullosa can be overlooked for years.
Once we confirm concha bullosa diagnosis with a careful exam, nasal endoscopy, and CT imaging, treatment becomes much clearer. Some people do well with medication. Others need a surgical approach such as crushing, outfracture, or endoscopic reduction, chosen carefully based on anatomy and safety concerns. When treatment matches the real cause, patients often feel a dramatic change in breathing and daily comfort.
If you have chronic nasal obstruction that has not responded to standard care, bring up concha bullosa during your ENT specialist consultation. When we name the problem correctly, we can finally choose the right concha bullosa symptoms treatment and help you breathe easier again.
Frequently Asked Questions
What is concha bullosa?
Concha bullosa is an air pocket inside a turbinate in your nose. Turbinates help warm, filter, and guide airflow. When one has an air cell inside it, the turbinate can become bulky and narrow the airway.
Is concha bullosa a disease?
No. It is an anatomic variation, not a disease. Many people have it without symptoms. It only becomes a problem when it blocks airflow or sinus drainage.
What do concha bullosa symptoms feel like?
Symptoms often feel like allergies or sinus trouble. You may notice constant nasal blockage, pressure, headaches, postnasal drip, or that one side of your nose never fully opens.
Can concha bullosa cause headaches?
Yes. Headaches may happen when the enlarged turbinate presses against nearby structures. This contact can trigger pain signals and feel like chronic or recurring sinus headaches.
Why does concha bullosa get missed?
Its symptoms overlap with allergies, sinusitis, and septal deviation. It may look like “normal anatomy” unless imaging and exam are carefully reviewed.
How do doctors diagnose concha bullosa?
Diagnosis is based on symptoms, nasal exam, nasal endoscopy, and a CT scan. CT imaging clearly shows the air pocket and how much space it takes up.
Does everyone with concha bullosa need treatment?
No. If you have no symptoms, no treatment is needed. Even large concha bullosa can be left alone if they do not cause problems.
Can medicine help concha bullosa symptoms?
Yes, in mild cases. Nasal sprays and other medications can reduce swelling and inflammation. They may improve symptoms but do not remove the air pocket itself.
When is surgery recommended?
Surgery is considered when symptoms persist despite medical treatment. It is most helpful when airflow or drainage is clearly blocked by the concha bullosa.
What does concha bullosa surgery involve?
Surgery is usually done endoscopically through the nose. Options include crushing or partially reducing the turbinate. The goal is to improve airflow while preserving normal nasal function.
Sources
- Toplu, Y., Bayindir, T., Karatas, E., & Akarcay, M. (2013). All concha bullosa: An undefined abnormality of the lateral nasal wall. Indian Journal of Otolaryngology and Head & Neck Surgery, 65(1), 86–88.
- Park, J.-H., Yi, K.-I., Cho, K.-S., & Kim, S.-D. (2019). A rare variant of middle turbinate extending to the nasal vestibule misinterpreted as nasal cavity tumor. Journal of Clinical Otolaryngology Head and Neck Surgery, 30(1), 97–99.
- Alnatheer, A. M., & Alkholaiwi, F. (2021). Concha bullosa of the inferior turbinate. Cureus.
- Cleveland Clinic. (2025, June 17). Concha bullosa.
- Mehta, R., & Kaluskar, S. K. (2011). Endoscopic turbinoplasty of concha bullosa: Long term results. Indian Journal of Otolaryngology and Head & Neck Surgery, 65(Suppl 2), 251–254.
Related Posts
Meniere’s Disease

About the Authors
