Chronic Sinus Infections Causes And Explanations For Persistent Symptoms

Millions of people live with what they’ve been told are “chronic sinus infections.” They take antibiotic after antibiotic. They try spray after spray. They still feel stuffed up, drained, and worn down.
If that sounds like you, I want you to know something important.
I have seen the same pattern for years. Patients walk into my ENT clinic with a grocery bag full of prescriptions. Some have tried just one more round of antibiotics so many times they lost count. They arrive frustrated and scared. They say, “Doc, my chronic sinusitis never goes away.”
Then I look at their CT scans. I see clear sinuses. No blockage. No thick mucus trapped inside the sinus cavities. Nothing that matches the label they were given.
Your symptoms are real, but your sinuses look fine, so what is really going on?
The cycle is costly. It drains your energy. It can lead to repeated antibiotic use, even when antibiotics are not the right tool. EPOS2020 also points out that rhinosinusitis is a common reason antibiotics are prescribed, and antibiotic resistance is a global crisis that makes proper management critical.
So let’s talk honestly about chronic sinus infections causes, and why some symptoms are actually not related to sinusitis.
Most “chronic sinus infections” aren’t infections
A true chronic condition is not a bad week or two. Chronic rhinosinusitis is tied to long-lasting inflammation in the nose and sinuses. It is not just a feeling of pressure. It is not just “I keep getting congested.”
In primary care and ENT care, the definition often comes down to symptoms that last at least 12 weeks, plus objective evidence on an exam or imaging. Objective evidence means I can see signs of inflammation. This might show up on a nasal exam with a scope or on a CT scan.
That “objective evidence” part is where many cases fall apart. People can have strong symptoms and still have no sign of sinus inflammation on imaging.
Symptoms alone can fool everyone
Sinus symptoms are not always sinus disease.
A study in a tertiary clinic looked at patients who had chronic rhinosinusitis symptoms and then had CT scans to check for inflammation. Many met symptom criteria, but symptoms alone did a poor job of separating true chronic rhinosinusitis from non-chronic rhinosinusitis. In plain terms, people can sound like sinusitis but not actually have it.
Even some classic complaints can mislead. In that same research, loss of smell was positively predictive for chronic rhinosinusitis, while facial pain was actually negatively predictive. That surprises many people. It also explains why chronic sinusitis misdiagnosis happens so often.
Why the system keeps mislabeling persistent symptoms
The medical system is busy, and sinus complaints are common.
EPOS2020 notes that rhinosinusitis is common worldwide and creates a large burden on health systems. When a problem is common, quick labels also become common.
Many patients describe pain, pressure, headache, and “sinus fullness.” Those words push the conversation toward infection. It feels logical. Yet symptom overlap is huge. Migraine, rhinitis, medication rebound, and nasal polyps can all mimic “sinus infection.”
Imaging often reveals the truth
When doctors suspect true chronic rhinosinusitis, we look for objective proof. CT can help confirm inflammation in the sinus cavities. It is also why patients are shocked when we say, “Your sinuses look clear.”
Nasal endoscopy is also powerful. One study found that adding nasal endoscopy to symptom criteria improved diagnostic accuracy and greatly increased specificity compared with symptoms alone. This helps avoid wrong treatments and unnecessary CT scans.
What really causes chronic sinus infections?
“Why do I always feel congested and drained?”
The answer is often not bacteria in the sinuses. The most common causes fall into a few big buckets.
Allergic rhinitis vs sinusitis
Allergic rhinitis can cause:
- Sneezing
- nasal congestion
- clear runny nose
- postnasal drip
- itching
It can also come with cough, Eustachian tube issues, and other symptoms that make people feel sick.
Allergic rhinitis is very common. It affects about one in six individuals and carries a major burden. People often assume thick symptoms mean infection. Yet allergic inflammation can be persistent and intense.
Triggers can also be sneaky. Patients may react to:
- pollens
- animal dander
- mold
- humidity
- perfumes
- tobacco smoke
- household exposures
When symptoms flare after exposure, it can look like another sinus infection, even though it’s an allergic pattern.
Chronic nonallergic rhinitis
Not all rhinitis is allergic. Chronic nonallergic rhinitis covers multiple subtypes that are not allergic and not infectious. It includes forms tied to:
- temperature shifts
- odors
- humidity
- food
- aging
- drugs
- hormones
- occupational triggers
This is a common reason for persistent nasal symptoms. Chronic nonallergic rhinitis represents about one-fourth of rhinitis cases and affects tens of millions of people in the United States.
That number alone explains why so many people get stuck in sinus infection treatment failure. They treat infection, but the real issue is a rhinitis subtype.
Migraine mistaken for “sinusitis”
A study of migraine patients who had a past history of sinusitis found that 81.5% were misdiagnosed as sinusitis. The average delay to the correct migraine diagnosis was 7.75 years, and some waited decades. Many had normal sinus investigations. When the diagnosis was corrected and treated as migraine, symptoms improved in 68.9%.
Why does this happen?
Because migraine can come with nasal symptoms, facial discomfort, and pressure sensations that people call “sinus pain.” In the symptom research on chronic rhinosinusitis, migraine-type features like throbbing pain and photophobia were negative predictors for true chronic rhinosinusitis.
That overlap is a major driver of chronic sinusitis misdiagnosis.
Nasal polyps and chronic inflammation
Nasal polyps are another common cause of nasal blockage and poor smell. They are benign inflammatory growths that can lead to:
- nasal obstruction
- congestion
- reduced quality of life
Patients with nasal polyps often report blockage, postnasal drip, facial pressure, and smell loss. That sounds like sinus infection to most people. While the presence of polyps is often associated with chronic sinusitis, it is typically a non-infectious variant and is thus managed very differently!
Diagnosis is supported by nasal endoscopy and imaging, usually CT, to assess extent and rule out other causes. Treatment often starts with intranasal corticosteroids and saline irrigation, and surgery can be needed in refractory cases.
Medication overuse rhinitis from decongestant sprays
Some of the worst nasal congestion I see is caused by the very sprays people use to fix congestion.
Rhinitis medicamentosa, also called rebound congestion, is inflammation caused by overuse of topical nasal decongestants. It can develop as early as 3 days and up to 4 to 6 weeks of use.
Patients then feel trapped. They spray to breathe. The effect shortens. They spray again. Congestion keeps returning.
The treatment is stopping the decongestant. Symptoms can worsen during withdrawal, so patients need clear counseling. Full recovery can take a long time in long-term overuse.
Environmental and occupational irritants
Chemical rhinitis and occupational rhinitis show up in differential lists for rhinitis. People may react to workplace exposures, household chemicals, or strong irritants. Even if you do not think of yourself as allergic, your nose can still respond with swelling, congestion, and runny drainage.
Hormonal causes
Hormonal rhinitis and rhinitis of pregnancy are also described in rhinitis differentials. If symptoms change with life stage or hormonal shifts, that pattern matters. It often points away from infection.
Why traditional sinus treatments keep failing you
When patients tell me they’ve tried everything, they usually mean antibiotics, decongestants, and occasional steroids. The problem is if the diagnosis is wrong, the treatment will miss.
Antibiotics often do not help, even in acute cases
Antibiotics are widely used for rhinosinusitis, but evidence for benefit can be limited. A randomized trial of adults with acute rhinosinusitis compared amoxicillin to placebo and found no significant symptom difference at day 3, and no meaningful difference at day 10. Some improvement showed at day 7, but overall the early relief many people expect did not happen.
So when someone with persistent sinus symptoms takes antibiotics and feels better later, the improvement may be timing. EPOS2020, as mentioned above, describes acute rhinosinusitis as usually self-limiting and often the consequence of a viral cold. Many people improve because the illness runs its course, not because the antibiotic killed it.
Antibiotic overuse is common
A cross-sectional study across multiple countries found that more than 80% of patients labeled with acute rhinosinusitis were prescribed antibiotics, and many did not meet guideline criteria. A large portion had symptoms for less than 5 days, yet antibiotics were still given. That pattern feeds the bIt can also come with cough, Eustachian tube issues, and other symptoms that make people feel sick.
symptoms equals antibiotic need,” even when the cause is viral, allergic, or something else.
EPOS2020 highlights that proper management matters in the context of global antibiotic resistance. If your condition is not bacterial, antibiotics add risk without solving the true problem.
Decongestant sprays can backfire
If you rely on topical decongestants too long, rebound congestion can become the main driver of symptoms. Rhinitis medicamentosa is literally caused by the medication. At that point, each spray gives short relief but deepens the cycle.
This is a major contributor to nasal congestion causes that look like chronic sinus disease. Yet it is treatable when identified.
Steroids can help, but they must match the condition
Intranasal corticosteroids have strong roles in allergic rhinitis management and are considered first-line therapy. They are also core therapy for chronic rhinosinusitis with or without nasal polyps.
But a steroid does not cure the root of every symptom. If the real issue is migraine, steroid sprays will not fix headache patterns. If the issue is rebound congestion from decongestant use, steroids can help during withdrawal, but stopping the decongestant spray is still essential.
This is why sinus infection treatment failure is so common. People rotate treatments without first locking down the right diagnosis.
How to finally identify what’s really causing your symptoms
You do not need to guess. You need clues.
Start with symptom patterns, not labels
Ask yourself questions about timing and triggers:
- Do symptoms flare with seasons?
- Do they worsen after dust, pets, mold, perfumes, or smoke exposure?
Allergic rhinitis history-taking focuses on type of symptoms, timing, frequency, suspected exposures, and seasonality. That approach works because patterns often reveal cause.
Also notice the type of drainage. Clear, thin drainage fits allergic rhinitis descriptions. Thick, discolored drainage can occur in other conditions, but color alone does not prove bacterial infection.
Pay attention to smell changes and headache features
Loss of smell is a symptom in chronic rhinosinusitis evaluation and was a positive predictor of chronic rhinosinusitis in the CT-based study mentioned above. So if smell loss is a major, ongoing issue, I take that seriously.
On the other hand, certain pain patterns can point away from chronic rhinosinusitis. Facial pain was negatively predictive for chronic rhinosinusitis in that same research, and throbbing pain with photophobia also pointed away. That does not mean pain is never sinus. It means pain alone is a shaky foundation for a sinus diagnosis.
Migraine misdiagnosis is also common. In the migraine study, most patients who carried a sinusitis label were actually migraine cases, and many had normal sinus investigations. If your sinus symptoms track with recurrent headache patterns, that is an important clue.
Know when imaging and endoscopy matter
A definitive diagnosis of chronic rhinosinusitis requires objective findings on endoscopy or CT. Symptoms are not enough. If you have had persistent symptoms for months and keep hearing “sinus infection”, it is reasonable to ask whether objective evidence has been found.
Endoscopy can be especially helpful. Adding endoscopy to symptom criteria improved specificity compared with symptoms alone in one study. That can reduce unnecessary imaging and sharpen treatment choices.
CT is commonly used for staging and assessment, but repeated CT scans raise concerns about cumulative radiation dose. A review notes MRI may be a complementary tool when repeated imaging is needed.
Red flags that should push you to specialist evaluation
Certain patterns should never be brushed off. There are conditions that require careful evaluation, such as possible cerebrospinal fluid leak with clear, refractory drainage, or concerning unilateral findings that raise concern for malignancy.
If something is one-sided, bloody, unusual, or persistent in a way that does not fit your normal pattern, it deserves a closer look.
Advocate for a real workup
If you are stuck, here is what I suggest you ask for:
- A focused history that looks at triggers, timing, and symptom type
- A nasal exam, and if available, nasal endoscopy
- A discussion of whether your symptoms meet chronic rhinosinusitis criteria and whether objective evidence is present
- If allergy is suspected and you do not respond to empiric therapy, consider allergy testing, which is described as useful for patients who do not respond or when identifying specific allergens is needed
How to get relief for persistent symptoms
Once you accept that “chronic sinus infection” might be the wrong name, you can finally choose treatments that match the real cause.
Step 1: Break the cycle of repeated antibiotics
If you have had multiple antibiotic courses without lasting relief, it is time to pause. Evidence for benefit is limited in many acute cases, and chronic rhinosinusitis is often described as an inflammatory process rather than a simple infection. EPOS2020 also stresses antibiotic stewardship in the context of resistance.
Step 2: Treat allergic and nonallergic rhinitis directly
For allergic rhinitis, intranasal corticosteroids are described as first-line therapy, and proper technique and regular use matter. Some patients also benefit from:
- antihistamines
- intranasal antihistamines
- leukotriene receptor antagonists
- immunotherapy (when needed)
If triggers are environmental, avoidance steps can help, though they are not always practical. Even pet dander clearance can take time, with one example noting cat dander may take up to 20 weeks to eliminate after removal.
For chronic nonallergic rhinitis, treatment is symptom-driven and often uses similar tools, including intranasal corticosteroid, plus trigger avoidance when possible. Furthermore, intranasal anticholinergics are often prescribed.
Step 3: If you have rebound congestion, stop the offending spray safely
For rhinitis medicamentosa, the core treatment is discontinuation of the topical decongestant. Congestion may temporarily worsen so they do not panic and restart. Intranasal corticosteroids may reduce rebound symptoms during withdrawal.
In long-term overuse, recovery can take a long time, with one study noting about a year for complete recovery. That timeline sounds scary, but many patients feel meaningful improvement long before complete recovery, especially once the cycle ends.
Step 4: Address nasal polyps and chronic inflammation with a plan
If nasal polyps are present, management often begins with intranasal corticosteroids and saline irrigation. If symptoms persist despite adequate therapy, surgery may be considered, with ongoing topical therapy still important afterward.
Long-term control and adherence are critical. Many patients relapse when they stop maintenance treatments too soon.
Step 5: If migraine is the real cause, treat migraine
If your sinus complaints are driven by migraine, relief can be dramatic once the diagnosis changes. In the migraine misdiagnosis study, most patients labeled as sinusitis were misdiagnosed, and migraine improved in 68.9% after proper diagnosis and treatment.
That is why I take headache features seriously and do not default to “sinus infection” based on facial discomfort alone.
What to expect once the diagnosis is right
Once the cause matches the treatment, the plan becomes simpler and more predictable:
- Allergic rhinitis treatments often need consistent use because steroid sprays can take days to reach peak effect
- Immunotherapy is long-term. Build-up can take months, and maintenance can last years
- Rebound congestion improves after stopping decongestants, but the first phase can feel worse, so support matters
- Nasal polyps often require ongoing management even after procedures
The timeline varies, but the direction finally makes sense.
Final words
If you have persistent sinus symptoms that never respond the way they “should,” the problem may not be your sinuses.
In my clinic, the most common reason people stay stuck is they were treated for an infection when the real issue was allergic rhinitis, chronic nonallergic rhinitis, rebound congestion from spray overuse, sinusitis with nasal polyps, or even migraine.
The symptoms feel like infectious sinusitis, so the label seems reasonable. Yet studies show symptom-based diagnosis can be unreliable, and objective testing like endoscopy and CT can reveal a very different truth.
If you feel trapped in sinus infection treatment failure, do not accept “chronic sinusitis” as the final word. Track your symptoms. Note triggers and timing. Ask whether objective evidence supports the diagnosis. Seek evaluation from a clinician who will look beyond the obvious and match treatment to the real cause.
That is how you move from guessing to getting real relief.
Frequently Asked Questions
Are most chronic sinus infections really infections?
No. Most ongoing sinus symptoms are not caused by bacteria. True chronic sinusitis requires ongoing inflammation that can be seen on exams or scans.
Why do I have sinus pressure if my CT scan is normal?
Pressure alone does not mean sinus disease. Migraines, allergies, nasal irritation, or spray overuse can cause the same feeling, even when sinuses are clear.
What actually causes true chronic sinusitis?
True chronic sinusitis is caused by long-term inflammation and blocked sinus drainage. Doctors must see this on a nasal exam or CT scan to confirm it.
Can allergies feel like a sinus infection?
Yes. Allergies cause swelling, congestion, and drainage that mimic sinus infections. But allergies are not infections and do not show sinus blockage on scans.
Why do antibiotics keep failing my “sinus infection”?
Because bacteria may not be the problem. Antibiotics don’t treat allergies, migraines, irritation, or rebound congestion, all of which are common causes of chronic symptoms.
Can nasal sprays make sinus symptoms worse?
Yes. Overusing decongestant sprays can cause rebound congestion. This creates constant blockage that feels like sinus disease but is medication-caused.
Is facial pain a strong sign of chronic sinusitis?
No. Facial pain in the absence of other nasal symptoms often points away from true chronic sinusitis. Migraines are a very common cause of facial pressure and headache.
What role do nasal polyps play?
Nasal polyps cause chronic inflammation and blockage. They are diagnosed with endoscopy or imaging, not symptoms alone, and need targeted treatment.
How do doctors confirm real chronic sinusitis?
They look for objective evidence using nasal endoscopy or CT scans. Symptoms must last 12 weeks and show visible inflammation.
What causes chronic sinus symptoms when scans are clear?
Most often allergies, nonallergic rhinitis, migraines, environmental irritation, or spray overuse, not infection.
Sources
- Fokkens, W. J., Lund, V. J., Hopkins, C., Hellings, P. W., Kern, R., Reitsma, S., Toppila-Salmi, S., Bernal-Sprekelsen, M., & Mullol, J. (2020). Executive summary of EPOS 2020 including integrated care pathways. Rhinology, 58(2), 82–111.
- Sedaghat, A. R. (2017). Chronic rhinosinusitis. American Family Physician, 96(8), 500–506.
- Hsueh, W. D., Conley, D. B., Kim, H., Shintani-Smith, S., Chandra, R. K., Kern, R. C., & Tan, B. K. (2012). Identifying clinical symptoms for improving the symptomatic diagnosis of chronic rhinosinusitis. International Forum of Allergy & Rhinology, 3(4), 307–314.
- Bhattacharyya, N., & Gilani, S. (2018). Prevalence of potential adult chronic rhinosinusitis symptoms in the United States. Otolaryngology–Head and Neck Surgery, 159(3), 522–525.
- Akhouri, S., & House, S. A. (2023). Allergic rhinitis. In StatPearls [Internet]. StatPearls Publishing.
- Al-Hashel, J. Y., Ahmed, S. F., Alroughani, R., & Goadsby, P. J. (2013). Migraine misdiagnosis as a sinusitis, a delay that can last for many years. The Journal of Headache and Pain, 14(1), Article 97.
- del Toro, E., Hardin, F. M. L., & Portela, J. (2025). Nasal polyps. In StatPearls [Internet]. StatPearls Publishing.
- Wahid, N. W. B., & Shermetaro, C. (2023). Rhinitis medicamentosa. In StatPearls [Internet]. StatPearls Publishing.
- Garbutt, J. M., Banister, C., Spitznagel, E., et al. (2012). Amoxicillin for acute rhinosinusitis: A randomized controlled trial. JAMA, 307(7), 685–692.
- Jørgensen, L. C., Christensen, S. F., Cordoba Currea, G., Llor, C., & Bjerrum, L. (2013). Antibiotic prescribing in patients with acute rhinosinusitis is not in agreement with European recommendations. Scandinavian Journal of Primary Health Care, 31(2), 101–105.
- Sedaghat, A. R. (2017). Chronic rhinosinusitis. American Family Physician, 96(8), 500–506.
- Garbutt, J. M., Banister, C., Spitznagel, E., et al. (2012). Amoxicillin for acute rhinosinusitis: A randomized controlled trial. JAMA, 307(7), 685–692.
Related Posts
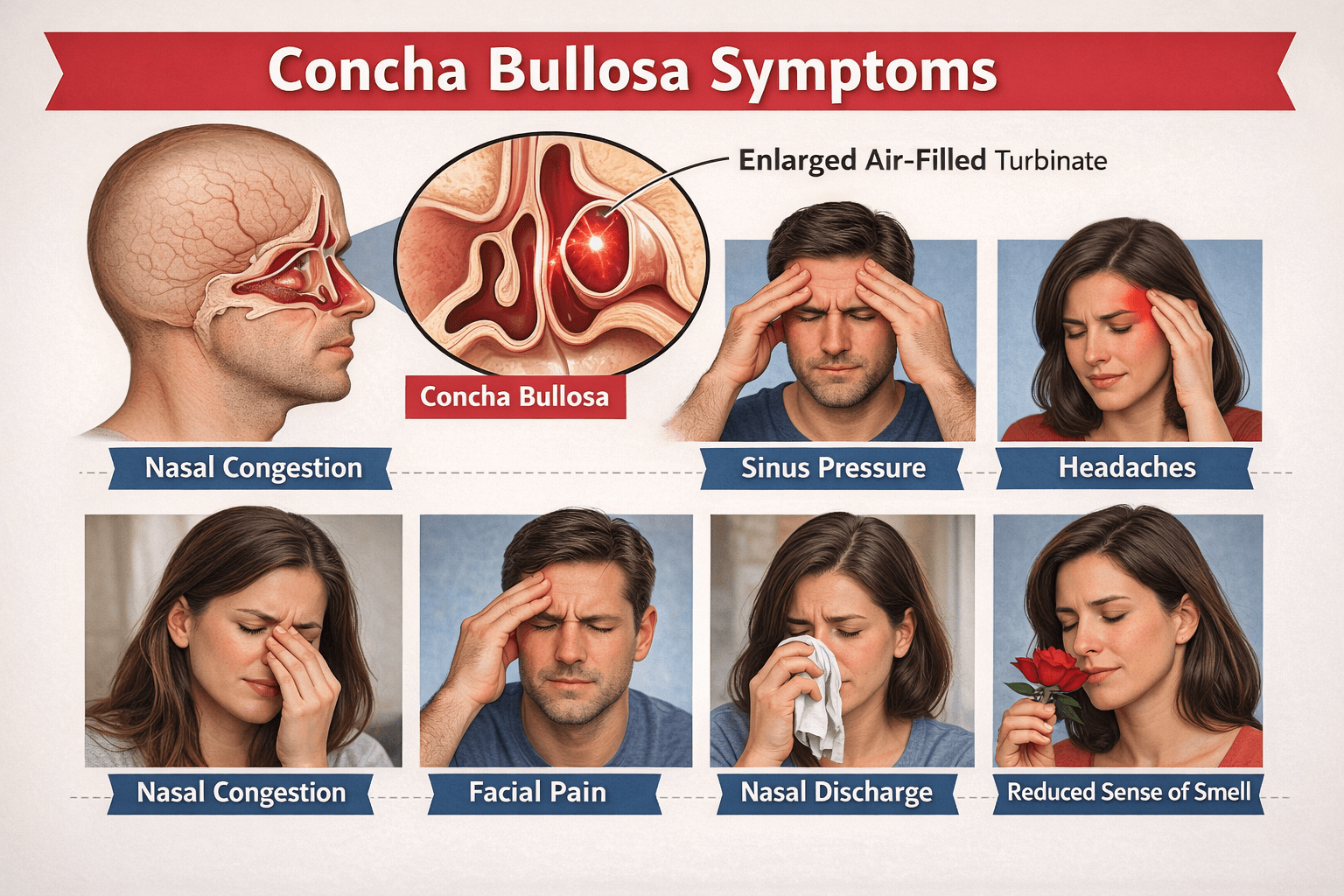
Concha Bullosa symptoms and treatment: How I explain it to my patients
About the Authors
