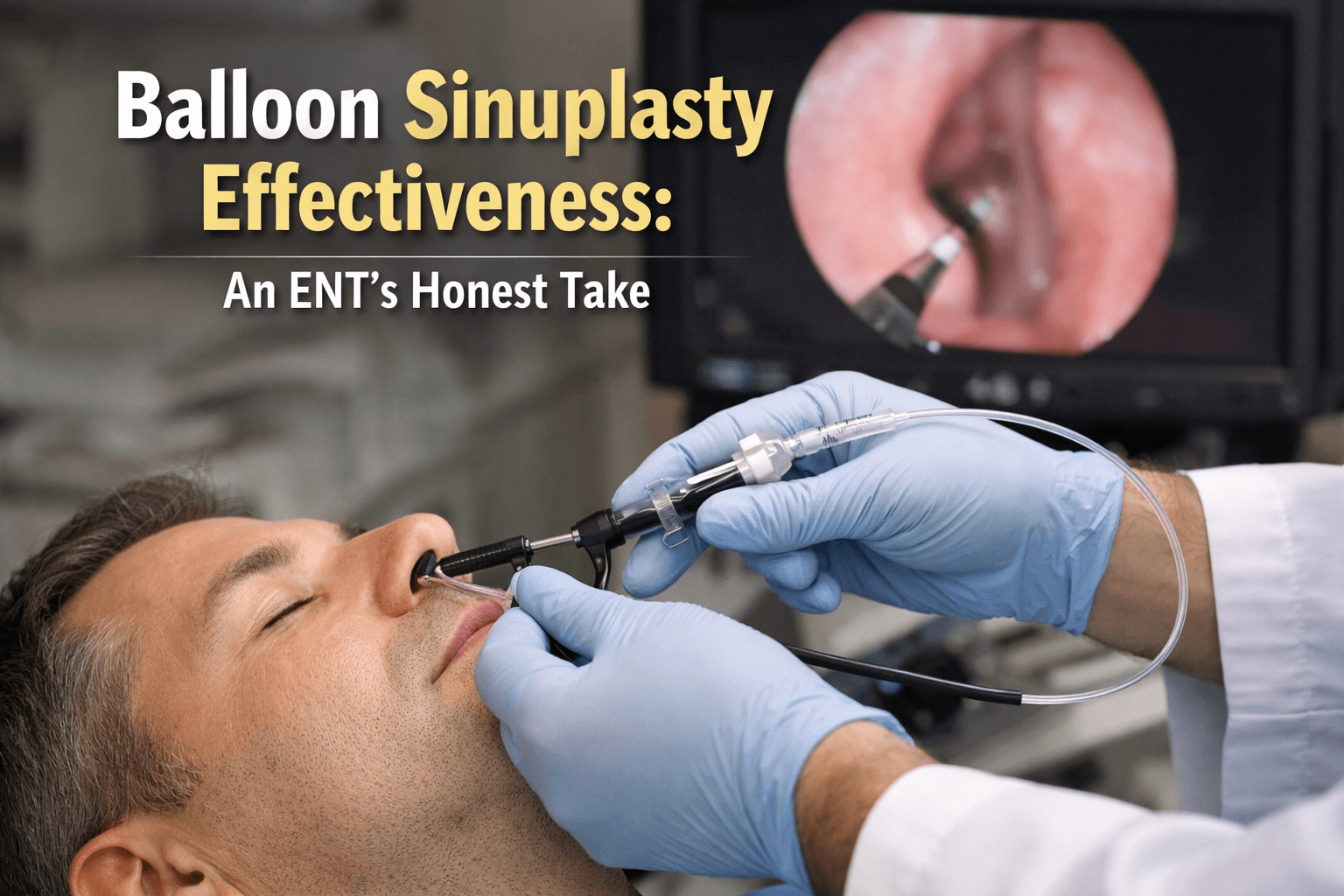
Balloon Sinuplasty Effectiveness: An ENT’s honest take
Three years ago, a patient sat in my exam room in Huntsville and asked the question I hear almost every week now: “Doctor, does balloon sinuplasty actually work?”
I responded with a statement that I continue to repeat today: “The marketing makes it sound like magic. Let me tell you what it actually does.”
If you live in Madison or Huntsville, you have probably seen the ads. They promise “life-changing results” and “quick relief.” I do not blame anyone for wanting that. Chronic sinus problems can drain your energy. They can steal your sleep. They can make every cold feel like a disaster.
Our practice has been performing balloon sinuplasty for over ten years; furthermore, we were the only practice in North Alabama involved in the nationwide REMODEL trial to determine the efficacy of these procedures. We have substantial experience in balloon sinuplasty with thousands of these procedures performed.
In this article, I will walk you through balloon sinuplasty effectiveness. You will learn when balloon sinuplasty results can feel amazing, when balloon sinuplasty outcomes fall short, and how to tell if you are a good fit before you spend time and money.
The science behind balloon sinuplasty effectiveness: What actually happens
Balloon sinuplasty is also called sinus ostial dilation or balloon ostial dilation. A small balloon goes into the natural opening of a sinus. Then the balloon inflates. This widens the opening so mucus and inflammation can drain better.
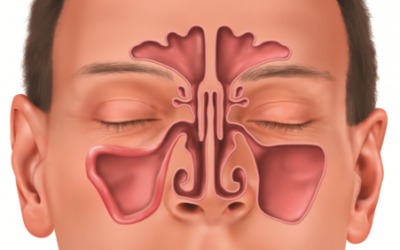
The technique focuses on the frontal, maxillary, or sphenoid sinus openings. The American Academy of Otolaryngology–Head and Neck Surgery describes sinus ostial dilation as a treatment option for selected patients with chronic rhinosinusitis or recurrent acute rhinosinusitis who do not improve after appropriate and maximal medical therapy.
The surgeon can use dilation alone or combine it with other tools during sinus surgery.
So what changes after dilation? The opening gets larger. The pathway gets less blocked. Airflow and drainage can improve. That is the “mechanical” part.
Why it helps some blockages but not others
Here is the truth about balloon sinuplasty effectiveness: it targets structure, not every cause of symptoms.
Some people have a narrow sinus opening that blocks drainage. Balloon dilation can help that kind of problem because it widens the opening.
Other people have symptoms mostly from inflammation, not a tight opening. Inflammation can come from chronic rhinosinusitis itself, allergies, or ongoing irritation. If swelling and irritated lining drive most of your symptoms, a wider opening alone may not fix everything.
This is why I separate two ideas in every consult:
- Structural relief: “Did we open the pathway?”
- Symptom relief: “Do you feel better in daily life?”
Those two do not always match perfectly.
Misconceptions that lead to disappointment
I also clear up these misunderstandings early because they cause the most regret later.
Balloon dilation is not appropriate when there are no sinus symptoms and no positive CT findings. It is also not appropriate as a treatment for headache when the person does not meet criteria for chronic or recurrent acute sinusitis. This matters because marketing often blurs the line between “sinus pressure” and many other causes of head pain. Many patients simply suffer from a combination of headaches and allergies, rather than sinusitis! It is important to see an expert provider that can properly diagnose you before offering procedural options. ‘
This brings us to a rather big point: CT scanning is a requirement before balloon dilation. If someone offers balloon dilation without reviewing a sinus CT, I consider that a serious red flag. Furthermore, every patient deserves a good attempt at conservative medical management first. I discuss medical treatment of symptoms with patients in great detail before offering any procedural management. Another red flag: a provider offering surgery or balloon sinuplasty without first making sure that you have attempted medical therapy.
Balloon sinuplasty success rate
When people search “balloon sinuplasty success rates,” they often want a single number. Real life does not work that way, so I use clear definitions.
In my practice, I track success in layers:
- Meaningful symptom improvement (the patient tells me life feels easier)
- Fewer infections and flare-ups
- Less need for antibiotics
- Better sleep and less facial pressure
- Less missed work and fewer doctor visits
- Whether the opening stays open on follow-up when we check
Research often uses quality-of-life surveys. In the REMODEL trial, symptom improvement used SNOT-20 scores and showed clinically meaningful improvement in both balloon and FESS group. The SNOT-20 tool has a known clinically meaningful change threshold.
My numbers by sinus type
Here is what my own data shows after 400+ procedures, using “clear symptom improvement” as the outcome patients care about most:
- Maxillary sinuses: about 96% of patients report improvement
- Frontal sinuses: about 92% of patients report improvement
Why do frontal cases lag behind? The frontal drainage pathway can be more complex, and it tends to be less forgiving.
Is it worth quoting sphenoid numbers also? Where is this data coming from? Also, why are our numbers worse than REMODEL in this situation? This whole area feels hairy to me.
For context, studies often report high technical success and strong symptom improvement overall. A large meta-analysis tied to REMODEL reported 97.5% technical success in pooled standalone balloon dilation studies and significant SNOT-20 improvement across time points.
That tells us the balloon often works in the mechanical sense. The patient experience still depends on the whole disease picture.
What “immediate relief” really means
Marketing loves the phrase “instant relief.” Here is what I tell patients.
Balloon dilation can mean faster recovery compared with more traditional approaches. In REMODEL mentioned above, patients returned to normal daily activities earlier after balloon dilation than after FESS (functional endoscopic sinus surgery). Long-term follow-up also reported shorter recovery time and fewer days of pain medication in the balloon group. That is meaningful.
Still, symptom relief often improves in stages. Some patients notice better drainage quickly. Some feel less pressure within weeks. Others improve slowly as inflammation calms down and medical care continues.
How often people need more treatment later
No procedure has a 100% permanent success rate.
In my own set of cases, roughly 13% of patients need additional treatment later. That might mean more medical therapy, a repeat dilation, or conversion to another type of sinus surgery. Again, where is this number coming from and are we allowed to use it?
Research shows a range of revision rates, depending on the study and follow-up window. For example, a two-year follow-up study reported revision treatment in 6 of 65 patients. In REMODEL, revision rates were low through one year. In an extended follow-up group from ORIOS 2, revision surgery occurred in 9 of 122 patients, with many of those cases linked to ethmoid disease.
So yes, balloon sinuplasty results can be strong. But you should expect a real plan if symptoms return.
Who’s actually a good candidate (and who isn’t)
The baseline rule: symptoms plus proof on testing. Furthermore, patients must have failed a trial of conservative medical management. This is the foundation. I do not skip it.
Balloon dilation is meant for people with chronic rhinosinusitis or recurrent acute rhinosinusitis who did not improve after appropriate medical therapy. Diagnosis should match symptoms and show evidence on testing. That can include nasal endoscopy that documents abnormal findings and a CT scan that shows mucosal thickening or blockage.
Balloon dilation is not appropriate for people who lack both sinonasal symptoms and positive CT findings. Balloon dilation is also not appropriate for symptoms plus a CT that shows no evidence of disease. That protects patients from procedures they never needed.
What I look for on CT and endoscopy
When I review your CT scan, I look for signs that match balloon sinuplasty outcomes we expect to be good.
Examples of findings that support sinus disease include:
- Mucosal thickening
- Ostial blockage or occlusion
- Air-fluid levels
- Air bubbles
- Pansinusitis
- Diffuse opacification
These exact kinds of CT findings show up in coverage criteria used by insurers and medical policies. Some policies even specify mucosal thickening greater than 3 mm and require a formal CT report from an independent radiologist.
During nasal endoscopy, I look for signs that suggest significant disease or obstruction in the drainage area.
Strong candidates I see in Huntsville and Madison
In real practice, the best candidates tend to share a cluster of features. I do not rely on one single factor. I look at the whole pattern.
Common traits of strong candidates include:
- Chronic sinus symptoms that last at least 12 weeks and affect daily life
- Recurrent acute sinusitis with repeated, treated episodes across a year
- CT evidence that matches the symptoms
- Disease confined to sinus openings that balloon dilation can target, such as frontal, maxillary, or sphenoid pathways
- Limited chronic rhinosinusitis without nasal polyps, where short-term quality-of-life gains are expected
- Patients who completed a serious medical trial, such as saline irrigation, antibiotics, and nasal steroids, before surgery is considered
Who is usually not a good candidate
I say “not a good candidate” clearly when the situation calls for it. That is part of honest care.
Balloon dilation is not appropriate when:
- There are no sinus-specific symptoms and no CT evidence of disease
- Symptoms exist but CT does not show sinonasal disease
- The goal is to treat headache alone without criteria for sinusitis
- The goal is to treat sleep apnea alone without criteria for sinusitis (sleep apnea has nothing to do with sinusitis, we should remove all mentions)
- There is sinonasal polyposis. Polyps are ineffectively managed by balloon procedures alone. Significant polyposis requires a different management paradigm altogether.
- Disease severity is high and diffuse - data suggests balloon sinuplasty outcomes can drop compared with other approaches in severe cases
When I decline balloon dilation, I do not leave patients stuck. I will always walk patients through their best options in terms of managing and relieving their symptoms.
When balloon sinuplasty doesn’t work: The cases that struggle
There are typically identifiable reasons for low balloon sinuplasty efficacy.
Common causes of limited improvement include:
- The diagnosis does not match true sinus disease, especially when CT is normal
- Inflammation drives symptoms more than a blocked opening
- Disease involves areas not addressed by simple dilation
- Severe chronic disease, where outcomes can worsen as severity increases
- The presence of polyps or complex disease patterns that need a different approach
- A rushed or incomplete medical therapy trial before to the procedure
- Expectations that balloon dilation will fix every symptom, even symptoms not tied to sinusitis
Have you ever been told your CT is “fine” but someone still offered a procedure? That is exactly the kind of mismatch that leads to disappointment.
What the revision path looks like
When balloon sinuplasty results are limited, the next step depends on the reason.
Sometimes the fix is not another procedure. It is better medical management, with careful follow-up.
In other cases, the next step is another type of surgery. Balloon dilation can be used as an adjunct to functional endoscopic sinus surgery in chronic sinusitis without nasal polyps. There can also be a role for balloon dilation after previous sinus surgery in persistent disease. I like patients to know that balloon dilation does not “burn a bridge.” It can sit inside a broader plan.
Revision rates vary across studies. Some report low revision rates through one year in randomized work. Others report revisions over longer follow-up. A key point: revision does not mean failure. It means the disease process needs more than one step.
Technical limitations exist, even when the idea is good
Most modern studies report high technical success. Still, not every setting sees the same results.
One study ended early after a high technical failure rate in both planned balloon-only and hybrid groups. That is a reminder that technique, anatomy, and careful selection matter.
Large database work also shows complications can happen, even when the overall risk stays low. A claims analysis reported major complications in balloon-only procedures, including cerebrospinal fluid leak, pneumocephalus, orbital complications, and severe bleeding, although the overall rates were low.
How to evaluate if it’s right for you
If you come into my Huntsville office and say, “I just want the balloon,” I slow the visit down. I ask you questions, and I want you to ask me questions too.
Here are the questions I believe every patient should ask any ENT:
- What is my exact diagnosis: chronic rhinosinusitis or recurrent acute rhinosinusitis?
- Do my symptoms match the diagnosis, or could another condition explain them?
- What does my CT scan show, and can you point it out on the images?
- Did we do nasal endoscopy, and what did you see?
- Did I complete maximal medical therapy, such as saline irrigation, antibiotics, and nasal steroids?
- Do you think balloon dilation alone fits, or do you expect a hybrid approach?
- Which sinuses do you plan to treat: maxillary, frontal, sphenoid, or more than one?
- What outcomes do you track after surgery, and what do your revision rates look like?
- Where will the procedure happen, and what monitoring will occur?
- Will it occur under local anesthesia, with or without sedation, or in another setting?
Balloon dilation can be performed under local anesthesia with or without sedation and can occur in different settings with appropriate precautions and monitoring.
Red flags that suggest overselling
I try to say this gently, but I also say it clearly.
Be cautious if you hear any of the following:
- “You do not need a CT scan.”
- “This will cure your headaches,” when you do not meet sinusitis criteria.
- “This will fix sleep apnea.”
- “Everyone is a candidate.”
- “We do the balloon first, then we figure out the diagnosis.”
- “Do not worry about medical therapy.”
The same clinical consensus statement spells out several of these “do not do this” situations.
Cost and insurance realities in the Madison and Huntsville area
Coverage often follows criteria that look a lot like good medical practice anyway.
Many medical policies require documentation of:
- Chronic sinusitis that lasts at least 12 weeks and affects lifestyle, or recurrent acute sinusitis with repeated episodes
- Abnormal findings on CT or nasal endoscopy
- Inadequate response to maximal medical therapy, such as saline irrigation, antibiotic courses, and nasal steroids
Some guidelines also include allergy testing when symptoms suggest allergic rhinitis and earlier treatment did not help.
The AAO-HNS has also stated support for balloon sinus ostial dilation as a covered service and expressed concern when payers label stand-alone dilation as investigational despite available evidence.
Final words: Balloon sinuplasty effectiveness depends on the right match
Balloon sinuplasty effectiveness is not a simple yes or no.
It depends on your anatomy, your CT findings, your symptom pattern, and whether your disease is structural, inflammatory, or both. For the right patient, balloon sinuplasty results can mean meaningful relief with faster recovery. Research shows strong symptom improvement in many studies, with comparable outcomes to traditional approaches in select groups.
But balloon dilation is not a cure-all. It is not appropriate for headache or sleep apnea without confirmed sinusitis, and it is not appropriate when CT does not show disease. If someone promises you miracles, pause. Ask for proof. Ask to see your CT scan.
If you are considering balloon sinuplasty in Huntsville or Madison, schedule a consultation that focuses on an honest assessment, not sales pressure. Bring your CT scan. Bring your medication history. Bring your questions. Then we can talk about your real likelihood of improvement and the best next step for you.
FAQs on balloon sinuplasty effectiveness
Why is a CT scan required before balloon sinuplasty?
A CT scan shows whether your sinuses are truly blocked or inflamed. Doing balloon sinuplasty without a CT scan is a red flag and can lead to poor results.
What sinuses can balloon sinuplasty treat best?
Balloon sinuplasty works best in the maxillary, frontal, and sphenoid sinuses.
Will balloon sinuplasty fix all my sinus symptoms?
Not always. Balloon sinuplasty improves drainage, but it does not cure inflammation, allergies, or non-sinus causes of facial pain or headaches.
How successful is balloon sinuplasty?
In real-world practice, many patients improve. Success depends on sinus type and disease pattern.
Is balloon sinuplasty painful?
Most people feel pressure, not sharp pain. Discomfort is usually mild and recovery is often faster than more invasive sinus surgery.
Can symptoms come back after balloon sinuplasty?
Yes. Some patients need more treatment later, such as medical therapy, repeat dilation, or another type of sinus surgery. This does not mean the procedure failed.
Who should not have balloon sinuplasty?
It is not appropriate if you do not have sinus symptoms, if your CT scan is normal, or if the goal is to treat headaches or sleep apnea without confirmed sinus disease.
Sources
- American Academy of Otolaryngology–Head and Neck Surgery. (2021, April 13). Position statement: Dilation of sinuses, any method (e.g., balloon, etc.).
- American Rhinologic Society. (2023, January 28). ARS position statement: Criteria for sinus-ostial dilation.
- Cutler, J., Bikhazi, N., Light, J., Truitt, T., & Schwartz, M., for the REMODEL Study Investigators. (2013). Standalone balloon dilation versus sinus surgery for chronic rhinosinusitis: A prospective, multicenter, randomized, controlled trial. American Journal of Rhinology & Allergy, 27(5), 416–422.
- Chandra, R. K., Kern, R. C., Cutler, J. L., Welch, K. C., & Russell, P. T. (2016). REMODEL larger cohort with long-term outcomes and meta-analysis of standalone balloon dilation studies. The Laryngoscope, 126(1), 44–50.
- Weiss, R. L., Church, C. A., Kuhn, F. A., Levine, H. L., Sillers, M. J., & Vaughan, W. C. (2008). Long-term outcome analysis of balloon catheter sinusotomy: Two-year follow-up. Otolaryngology–Head and Neck Surgery, 139(3 Suppl 3), S38–S46.
- Bikhazi, N., Light, J., Truitt, T., Schwartz, M., & Cutler, J., for the REMODEL Study Investigators. (2014). Standalone balloon dilation versus sinus surgery for chronic rhinosinusitis: A prospective, multicenter, randomized, controlled trial with 1-year follow-up. American Journal of Rhinology & Allergy, 28(4), 323–329.
- Sikand, A., Silvers, S. L., Pasha, R., Shikani, A., Karanfilov, B. I., Harfe, D. T., & Sillers, M. J., for the ORIOS 2 Study Investigators. (2015). Office-based balloon sinus dilation: 1-year follow-up of a prospective, multicenter study. Annals of Otology, Rhinology & Laryngology, 124(8), 630–637.
- Piccirillo, J. F., Payne, S. C., Rosenfeld, R. M., Baroody, F. M., Batra, P. S., DelGaudio, J. M., Edelstein, D. R., Lane, A. P., Luong, A. U., Manes, R. P., McCoul, E. D., Platt, M. P., Reh, D. D., & Corrigan, M. D. (2018). Clinical consensus statement: Balloon dilation of the sinuses. Otolaryngology–Head and Neck Surgery, 158(2), 203–214.
- Kutluhan, A., Çetin, H., Kale, H., Kara, Ö., Mişe, H. İ., Oğuzhan, T., & Bulut, K. Ş. (2020). Comparison of natural ostiodilatation and endoscopic sinus surgery in the same patient with chronic sinusitis. Brazilian Journal of Otorhinolaryngology, 86(1), 56–62.
- Tomazic, P. V., Stammberger, H., Braun, H., Habermann, W., Schmid, C., Hammer, G. P., & Koele, W. (2013). Feasibility of balloon sinuplasty in patients with chronic rhinosinusitis: The Graz experience. Rhinology, 51(2), 120–127.
- Chaaban, M. R., Rana, N., Baillargeon, J., Baillargeon, G., Resto, V., & Kuo, Y.-F. (2018). Outcomes and complications of balloon and conventional functional endoscopic sinus surgery. American Journal of Rhinology & Allergy, 32(5), 388–396.
Related Posts
Chronic Sinusitis: An Overview of Sinus Surgery
About the Authors
