Allergic vs non-allergic rhinitis: What we have learned after over 20 years as an ENT medical practice

I still remember a visit that changed the way I explain chronic congestion.
I was sitting across from a patient who looked tired. They had tissues in both hands. They told me, “I know it’s allergies. It has to be.” I pulled up a chart I often use in clinic and said something I say almost every week now: most people walk in convinced they have allergies, but many adults, especially as they get older, actually have non-allergic rhinitis. The treatments are not the same. When you treat the wrong type, you can feel stuck for years.
Rhinitis is very common. It shows up as at least one of these symptoms: congestion, runny nose (rhinorrhea), sneezing, nasal itching, or nasal blockage. Some people also get throat clearing, headaches, facial pain, ear pain, an itchy throat or palate, snoring, and sleep problems. The hard part is that allergic vs. non-allergic rhinitis can look similar at first.
So how do you tell?
I will walk you through the differences in allergic vs non-allergic rhinitis, with a special focus on something many people miss: age patterns and nerve-based triggers.
I will also show you how trigger clues and treatment response can point you toward the right diagnosis.
The age pattern that changes everything: When allergic vs non-allergic rhinitis usually shows up
Age does not prove what type you have. Still, the rhinitis age pattern often gives me my first big clue.
Allergic rhinitis is extremely common. In the United States, it affects about 10–30% of adults and up to 40% of children. It also has clear allergen links. Seasonal allergic rhinitis often relates to pollens that vary by region. Perennial allergic rhinitis often relates to dust mites, mold spores, and animal dander.
Non-allergic rhinitis is also common, but people talk about it less.
It is usually described as chronic nasal symptoms, often obstruction and runny nose, that happen with non-allergic, non-infectious triggers like weather changes, caustic odors, cigarette smoke, and barometric pressure shifts.
What I see in real life: Adults often shift over time
A lot of patients do not have only one type. In fact, 44% to 87% of people with rhinitis can have mixed allergic and non-allergic rhinitis. Sneezing does not always mean “pure allergy.”
So what does the age pattern look like in practice?
In a large review of records from a managed care program, people with non-allergic rhinitis were older on average than people with allergic rhinitis. The mean age was 42.6 for non-allergic rhinitis versus 35.8 for allergic rhinitis. Non-allergic rhinitis patients were also more likely to be female.
Some describe non-allergic rhinitis as something that often appears later in life. For example, vasomotor rhinitis, the most common form of non-allergic rhinitis, is described as developing most commonly between the ages of 30 and 60.
A validated questionnaire approach also highlighted that symptom onset after age 35 can strongly point toward vasomotor rhinitis when paired with other features like symptom triggers from perfumes and fragrance.
The “switch” that should make you pause
Here is a pattern that is always heard:
- “I used to get symptoms only in certain months.”
- “Now I feel congested most days.”
- “Allergy pills used to help. Now they barely touch it.”
When symptoms shift from seasonal to more constant, it becomes important to look harder for non-allergic triggers or mixed rhinitis. A person can still have allergies. But they may also develop strong non-allergic triggers on top of it. That is when same old allergy treatment stops feeling reliable.
The nerve connection: Why non-allergic rhinitis often feels so random
Many people think rhinitis is always an immune problem. That is true for allergic rhinitis, but it is not the whole story.
Allergic rhinitis is an IgE-mediated disease. It causes inflammation in the nasal lining. Allergic patients have more allergen-specific IgE in the nasal mucosa. Histamine release from mast cells plays a major role. Eosinophils also matter. A Th2 response follows, with cytokines like IL-4 and IL-5 involved. There is also an immediate phase and a late phase, and congestion tends to stand out in the late phase.
Non-allergic rhinitis can work differently. In many patients, it functions largely as nerve based rhinitis, with symptoms driven by autonomic nervous system dysregulation and hypersensitive nasal nerves rather than classic immune inflammation.
The nose has “wiring” that controls swelling and mucus
Your nose has blood vessels and glands. Nerves help control both.
- The parasympathetic nervous system promotes gland activity. It increases watery secretions. It releases acetylcholine.
- The sympathetic nervous system tightens blood vessels. This reduces swelling in the nasal lining. Nasal decongestants that stimulate alpha-adrenergic receptors can reduce mucosal thickness.
In vasomotor rhinitis, the problem is often described as a dysregulation of sympathetic, parasympathetic, and nociceptive nerves that innervate the nasal mucosa. When parasympathetic signals dominate, mucus secretion can rise. When vascular tone shifts, congestion can rise. The result can feel unpredictable.
Sensory nerves react to the world around you
The nasal lining also has sensory nerve fibers.
- Thin Aδ fibers send signals like pain and cold to the brain.
- C fibers conduct signals more slowly, and they react to many irritants. Cigarette smoke, nicotine, aldehyde, formaldehyde, isocyanates, sulfur dioxide, and other toxicants can stimulate them.
This matters because many non-allergic triggers are not “allergens.” They are irritants or environment shifts that set off nerve responses.
Capsaicin, the chemical in spicy peppers, is famous here. It activates certain receptor and ion channel proteins. Some sensations can also rise when osmotic tonicity changes quickly at the cell surface.
This can happen when dry pollen and dust land on mucosal surfaces and water moves out of epithelial cells. The feeling can be intense even if allergy tests are negative.
What research shows about nerve involvement
Autonomic dysfunction has been studied directly in vasomotor rhinitis. In one study, patients with vasomotor rhinitis had significant abnormalities on autonomic nervous system testing compared with control.
That supports what many patients describe: their nose overreacts to “normal” things.
Trigger patterns: How to tell which type of rhinitis you might have
This is the part I love teaching, because it gives you real control. You do not need to guess. You can look for patterns.
Allergic rhinitis triggers tend to be specific
Allergic rhinitis symptoms happen when an allergen triggers them. The trigger often includes:
- dust mites
- mold spores
- animal dander
- pollens that vary by region, including trees, grasses, weeds, and more
People often notice seasonal timing. Others have symptoms all year if the trigger is always around.
It is also common for allergic rhinitis to come with eye symptoms, since the same allergic process can affect the eyes. Many patients also have other allergic disease in the background.
Non-allergic rhinitis triggers can be broad and “everyday”
Non-allergic rhinitis is linked to non-allergic, non-infectious triggers. Common examples include:
- weather change
- cold air
- shifts in temperature and humidity
- barometric pressure differences
- strong odors like perfumes, soaps, paint, and cleaning supplies
- cigarette smoke and tobacco smoke
- air pollutants and chemical irritants
- exercise
- alcohol ingestion
- hot or spicy foods, especially in gustatory rhinitis
Some subtypes have very specific clues. Gustatory rhinitis appears after eating, especially hot or spicy foods. Drug-induced rhinitis includes rhinitis medicamentosa, which can happen after repeated use of topical nasal decongestants like oxymetazoline or phenylephrin. Hormone-induced rhinitis can occur with endogenous female hormones such as pregnanc.
Do you notice non-allergic rhinitis symptoms after perfume exposure? After a temperature change? After cleaning a room? Those clues matter!
Why allergy tests can be negative in non-allergic rhinitis
A classic feature of non-allergic rhinitis is the lack of allergic disease on testing.
That often shows up as a negative skin prick test for relevant allergens or negative allergen-specific antibody tests. This is part of why people get misdiagnosed.
One expert described a common situation: patients with non-allergic rhinitis often get treated first with oral second-generation antihistamines. These are usually not enough. Then patients go through repeated treatment failures and frustration.
A simple symptom diary
You can do this on paper or in your phone. Track for at least 2 weeks:
Write down:
- Date and time symptoms start
- Main symptom: congestion, runny nose, sneezing, itch, postnasal drip, headache, sleep issues
- Where you were: bedroom, outdoors, car, workplace
- What happened right before: weather shift, cold air, shower, cleaning supplies, perfume, smoke, exercise, spicy meal, alcohol, medication use
- What helped: oral antihistamine, nasal spray, saline, decongestant, nothing
Treatment approaches: Why one-size-fits-all fails
If you treat allergic rhinitis like non-allergic rhinitis, or the other way around, you can waste a lot of time.
Rhinitis has a real burden. Direct medical costs and lost productivity add up. In the United States, direct medical costs for allergic rhinitis nearly doubled from $6.1 billion in 2000 to $11.2 billion in 2005. People also lose workdays and school days due to symptoms.
So getting this right really matters.
Treatments that target allergic rhinitis
Allergic rhinitis treatment often includes:
- allergen avoidance when possible
- oral and intranasal antihistamines
- intranasal corticosteroids
- intranasal cromones
- leukotriene receptor antagonists
- immunotherapy
First-generation antihistamines can cause sedation and anticholinergic side effects like dry mouth, urinary retention, constipation, and tachycardi. Second-generation antihistamines have less sedation overall, though some still cause it at higher doses.
Intranasal corticosteroids are described as the most effective medications for controlling all rhinitis symptoms. They work best with regular use. Side effects like crusting, dryness, and minor nosebleeds can happen, but technique can reduce this.
Immunotherapy can help when IgE-mediated triggers are clearly identified. It can also have long-lasting benefits.
Treatments that often help non-allergic rhinitis
Non-allergic rhinitis has multiple subtypes, including nonallergic rhinopathy (vasomotor rhinitis), NARES, atrophic rhinitis, senile rhinitis, gustatory rhinitis, drug-induced rhinitis, hormonal-induced rhinitis, and cerebrospinal fluid leak.
1. Intranasal corticosteroids
Intranasal corticosteroids are the mainstay of treatment for non-allergic rhinitis.
In a randomized trial, fluticasone propionate improved symptoms in perennial non-allergic rhinitis compared with placeb. Still, some subgroups may not respond well, especially weather-sensitive cases.
2. Topical antihistamines
Topical antihistamines can be very effective in non-allergic rhinitis. Azelastine has evidence for benefit in vasomotor rhinitis symptom scores.
In an open-label study, azelastine improved multiple symptoms across allergic rhinitis, mixed rhinitis, and non-allergic vasomotor rhiniti. Some people notice a metallic or bitter taste, and it often decreases over time.
3. Topical anticholinergics
Topical anticholinergics matter when watery rhinorrhea is the main issue. Ipratropium bromide nasal spray is recommended for rhinorrhea, including gustatory rhinitis. Combination therapy with an intranasal corticosteroid can work better than either alone for rhinorrhea.
4. Nasal saline irrigation
Nasal saline irrigation can help as an adjunct. A Cochrane review found favorable evidence for saline as an add-on therapy for chronic symptoms, with minor side effects like burning or irritation.
In another trial, large-volume, low-pressure saline irrigation improved symptom scores more than saline sprays.
5. Decongestants
Decongestants can relieve congestion, but it should be used carefully. Rebound congestion can happen with topical decongestants in some people after only a few days. That rebound problem is part of rhinitis medicamentosa.
Investigational options
Investigational options aboutr non-allergic rhinitis include:
- intranasal capsaicin
- silver nitrate
- acupuncture
Capsaicin showed long-term symptom reduction in a placebo-controlled study. Silver nitrate improved patient-reported symptoms in trials. Acupuncture showed symptom score changes in a randomized placebo-controlled pilot study for vasomotor rhinitis.
Here’s a summary comparing allergic vs non-allergic rhinitis:
Final words: The right label leads to real relief
The difference between allergic vs. non-allergic rhinitis often decides whether your treatment works.
Allergic rhinitis is tied to allergen-triggered, IgE-mediated inflammation. Non-allergic rhinitis often links to non-allergic triggers like weather changes, irritants, strong odors, and smoke, and it often involves nerve and autonomic pathways. Age patterns can also guide your thinking, since non-allergic rhinitis patients tend to be older on average in real-world data.
So ask yourself: do your symptoms line up with pollen and pets, or do they flare with cold air, perfume, smoke, pressure shifts, cleaning products, spicy foods, alcohol, or certain medicines? Did allergy treatment stop helping? Did testing come back negative?
If you have treated your congestion like allergies without success, especially if you are over the mid-30s to 40s range or you notice strong irritant triggers, it is worth looking harder at non-allergic rhinitis or mixed rhinitis.
Track your symptoms and triggers for a couple of weeks, then bring that record to an ENT visit. A clear history, paired with the right testing when needed, can finally move you from trial-and-error to targeted relief.
FAQs on allergic vs non-allergic rhinitis
How do you know if you have allergic vs non allergic rhinitis?
Start with patterns. Allergic vs non allergic rhinitis often looks similar, but triggers tell the story. If symptoms follow pollen, pets, or dust and testing is positive, allergies are likely. If symptoms flare with cold air, perfume, smoke, or weather changes and tests are negative, non-allergic rhinitis is more likely. Age of onset and treatment response also help clarify the diagnosis.
What does non-allergic rhinitis actually mean?
Non-allergic rhinitis means your nose reacts without an allergy or infection. Symptoms include congestion and a watery runny nose. The cause is often nerve-based rhinitis, where sensitive nasal nerves overreact to everyday triggers like temperature shifts, odors, or smoke. Allergy tests are usually negative.
Can a cold turn into non-allergic rhinitis?
Yes. A viral infection can start symptoms, but in some people, nasal nerves stay overactive even after the infection clears. This can look like ongoing non-allergic rhinitis rather than repeated infections or allergies.
How is allergic rhinitis confirmed?
Allergic rhinitis is confirmed with skin prick testing or blood tests that detect allergen-specific IgE. If testing is unclear or cannot be done, doctors rely on history, symptom patterns, and exam findings. Positive tests plus matching triggers support the diagnosis.
Can non-allergic rhinitis be misdiagnosed as allergies?
Yes, and it happens often. Rhinitis misdiagnosis is common when symptoms are assumed to be allergic without testing. Many patients are treated for years with allergy pills that stop working because the underlying problem is nerve-driven, not immune-driven.
Do allergies cause headaches in children?
They can. Allergic rhinitis may cause sinus congestion, which can lead to pressure and headaches. These headaches usually come with sneezing, nasal congestion, and itchy or watery eyes.
How can you tell if a headache is from allergies?
Allergy-related headaches often appear with nasal congestion, sinus pressure, sneezing, and itchy eyes. If headaches follow allergy seasons or exposure to known allergens, allergies are more likely involved.
Sources
- Tran, N. P., Vickery, J., & Blaiss, M. S. (2011). Management of rhinitis: Allergic and non-allergic. Allergy, Asthma & Immunology Research, 3(3), 148–156.
- Wallace, D. V., Dykewicz, M. S., Bernstein, D. I., Blessing-Moore, J., Cox, L., Khan, D. A., Lang, D. M., Nicklas, R. A., Oppenheimer, J., Portnoy, J. M., Randolph, C. C., Schuller, D., Spector, S. L., & Tilles, S. A. (2008). The diagnosis and management of rhinitis: An updated practice parameter. Journal of Allergy and Clinical Immunology, 122(2 Suppl), S1–S84.
- Schatz, M., Zeiger, R. S., Chen, W., Yang, S.-J., Corrao, M. A., & Quinn, V. P. (2008). The burden of rhinitis in a managed care organization. Annals of Allergy, Asthma & Immunology, 101(3), 240–247.
- Brandt, D., & Bernstein, J. A. (2006). Questionnaire evaluation and risk factor identification for nonallergic vasomotor rhinitis. Annals of Allergy, Asthma & Immunology, 96(4), 526–532.
- Jaradeh, S., Smith, T. L., Torrico, L., Prieto, T., & colleagues. (2000). Autonomic nervous system evaluation of patients with vasomotor rhinitis. The Laryngoscope, 110(11), 1828–1831.
- Ledford, D. K. (2003). Inadequate diagnosis of nonallergic rhinitis: Assessing the damage. Allergy and Asthma Proceedings, 24(3), 155–162. Retrieved from National Center for Biotechnology Information (NCBI):
- Sur, D. K. C., & Plesa, M. L. (2018). Chronic nonallergic rhinitis. American Family Physician, 98(3), 171–176. Retrieved from American Academy of Family Physicians (AAFP):
- Webb, D. R., Meltzer, E. O., Finn, A. F., Jr., Rickard, K. A., Pepsin, P. J., Westlund, R., & Cook, C. K. (2002). Intranasal fluticasone propionate is effective for perennial nonallergic rhinitis with or without eosinophilia. Annals of Allergy, Asthma & Immunology, 88(4), 385–390.
- Jacobs, R. L., Lieberman, P., Kent, E., Silvey, M., Locantore, N., & Philpot, E. E. (2009). Weather/temperature-sensitive vasomotor rhinitis may be refractory to intranasal corticosteroid treatment. Allergy and Asthma Proceedings, 30(2), 120–127.
- Harvey, R., Hannan, S. A., Badia, L., & Scadding, G. (2007). Nasal saline irrigations for the symptoms of chronic rhinosinusitis. Cochrane Database of Systematic Reviews, (3), CD006394.
- Pynnonen, M. A., Mukerji, S. S., Kim, H. M., Adams, M. E., & Terrell, J. E. (2007). Nasal saline for chronic sinonasal symptoms: A randomized controlled trial. Archives of Otolaryngology–Head & Neck Surgery, 133(11), 1115–1120.
- Blom, H. M., Van Rijswijk, J. B., Garrelds, I. M., Mulder, P. G., Timmermans, T., & Gerth van Wijk, R. (1997). Intranasal capsaicin is efficacious in non-allergic, non-infectious perennial rhinitis: A placebo-controlled study. Clinical & Experimental Allergy, 27(7), 796–801.
- Erhan, E., Külahli, I., Kandemir, O., Cemiloglu, R., Yigitbasi, O. G., & Cüreoglu, S. (1996). Comparison of topical silver nitrate and flunisolide treatment in patients with idiopathic non-allergic rhinitis. Tokai Journal of Experimental and Clinical Medicine, 21(2), 103–111. Retrieved from National Center for Biotechnology Information (NCBI):
- Schatz, M., Zeiger, R. S., Chen, W., Yang, S.-J., Corrao, M. A., & Quinn, V. P. (2008). The burden of rhinitis in a managed care organization. Annals of Allergy, Asthma & Immunology, 101(3), 240–247.
Related Posts
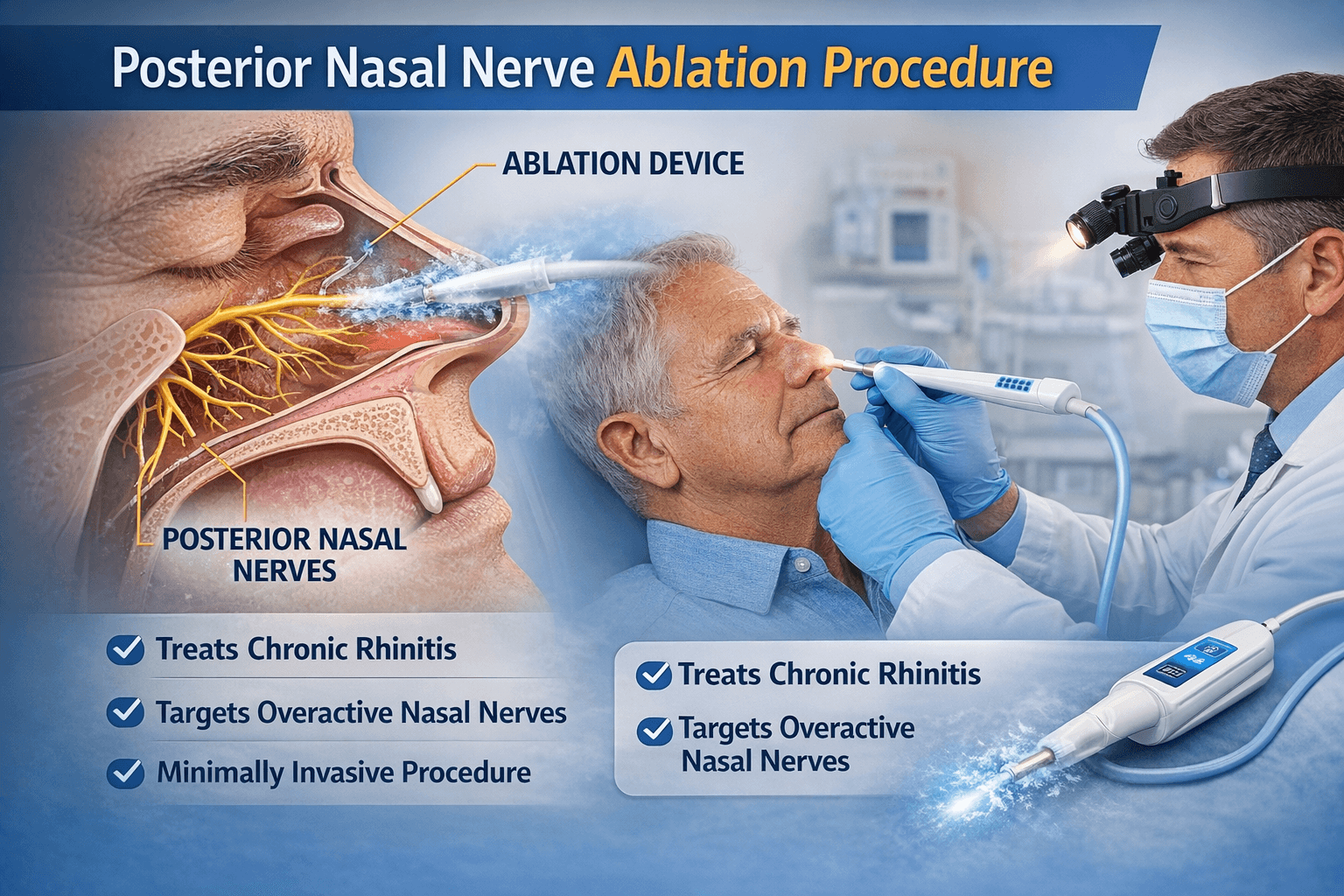
How the Posterior Nasal Nerve Ablation Procedure Changed My Patient’s Life
About the Authors
